|
|
|
   |
|
| CASE REPORT | |
|
Neutral zone concept applied in implant-supported mandibular complete denture treatment of a retrognathic patient
Diogo Longhini, Cibele Oliveira de Melo Rocha, Rodrigo de Paula Pereira, Gelson Luis Adabo, João Neudenir Arioli Filho
Department of Dental Materials and Prosthodontics, Araraquara Dental School, Universidade Estadual Paulista, Araraquara, São Paulo, Brazil
| Date of Web Publication | 15-Feb-2018 |
Correspondence Address:
Dr. Diogo Longhini
Department of Dental Materials and Prosthodontics, Universidade Estadual Paulista, Humaitá Street, 1680, Araraquara, São Paulo, Zip Code: 14801-903
Brazil
Source of Support: None, Conflict of Interest: None
 |
Check |
DOI: 10.4103/jdi.jdi_2_17

 Abstract Abstract |
This case report demonstrates the neutral zone technique for oral rehabilitation of patient with severe retrognathism, who had a previous implant-supported complete denture with improper relationship between artificial teeth and oral structures. A new mandibular screw-retained implant-supported complete denture was made base-on neutral zone principles to give to the patient a comfortable and functional prosthesis. The nonfunctional position of artificial teeth in complete denture may impair in oral functions such as speaking, swallowing, smiling, as well as loss of denture retention and stability, discomfort, and injuries to oral soft tissues. Neutral zone concept aids to produce complete denture more suitable, once it harmonizes the prosthesis to anatomic structures. In implant-supported complete dentures, retention and stability problems are not a concern. However, in some situations, nonfunctional artificial teeth position causes oral lesions, discomfort, and phonetics problems. Although neutral zone is a technique developed for conventional complete denture, it can be useful in implantology.
Keywords: Dental implants, dental prosthesis, dental prosthesis implant-supported, prosthodontics
| How to cite this article: Longhini D, de Melo Rocha CO, Pereira Rd, Adabo GL, Arioli Filho JN. Neutral zone concept applied in implant-supported mandibular complete denture treatment of a retrognathic patient. J Dent Implant 2017;7:59-63 |
| How to cite this URL: Longhini D, de Melo Rocha CO, Pereira Rd, Adabo GL, Arioli Filho JN. Neutral zone concept applied in implant-supported mandibular complete denture treatment of a retrognathic patient. J Dent Implant [serial online] 2017 [cited 2018 Mar 28];7:59-63. Available from: http://www.jdionline.org/text.asp?2017/7/2/59/225407 |
| Introduction |
Oral functions such as speech, mastication, and swallowing involve the combined action of the muscles of the tongue, lips, cheeks, and mouth floor,[1] and neuromuscular forces vary in magnitude and directions among individuals and age.[2] An equilibrium zone among resultant forces of those buccal muscles determines the position of the natural tooth.[3] Over the years, several authors contributed to the development of the neutral zone concept [1],[2],[4],[5],[6],[7],[8] which states that the denture should be placed where the forces between the lips and the cheeks are neutralized by the tongue forces during normal neuromuscular function.[2] The correct buccolingual arrangement of the artificial teeth in the neutral zone is essential to allow harmonious interaction between involved muscles in normal function and the prosthesis [1],[2],[7],[8],[9],[10],[11] which may prevent lack of retention and stability, discomfort and oral damages.[5],[12],[13],[14],[15],[16] Although this technique is mainly indicated to patients with highly atrophic ridges,[17] the neutral zone technique may be advantageous for fabricating most of the complete denture.[18]
Despite this technique has been known for a long time for removable complete dentures, it is not usually applied for implant-supported mandibular complete denture because problems such as retention and stability are not a concern. Nevertheless, applying the neutral zone technique make this prosthesis more functional and comfortable,[17] mainly in cases for patients who have higher overjet, where the mismatch between the position of artificial teeth and anatomic structures can affect oral functions and patient’s comfort.
This case report describes the use of neutral zone technique for making a new mandibular screw-retained implant-supported complete denture for a patient with severe retrognathism, who had a previous implant-supported complete denture that provoked oral injuries, phonetic problems, and discomfort.
| Case Report |
A 64-year-old man with a maxillary conventional complete denture and a mandibular screw-retained implant-supported complete denture [Figure 1] reported discomfort, injuries in buccal sulcus, phonetic problems, and difficult cleaning under the mandibular prosthesis.
 |
Figure 1: Intraoral view at the first appointment. There were some injuries in buccal sulcus caused by the overextension of the mandibular prosthesis |
Clinical examination showed a gingival over-extension of the labial border of the mandibular implant-supported complete denture and excessive buccal positioning of the artificial teeth to compensate the severe mandibular retrognathism, to give him Angle Class I occlusion. In addition, the prosthesis design [Figure 2] generated discomfort and phonetic difficulties because of limitation in lower lip movements and made difficult to perform appropriated oral hygiene. The maxillary removable complete denture was satisfactory from a functional and esthetic perspective.
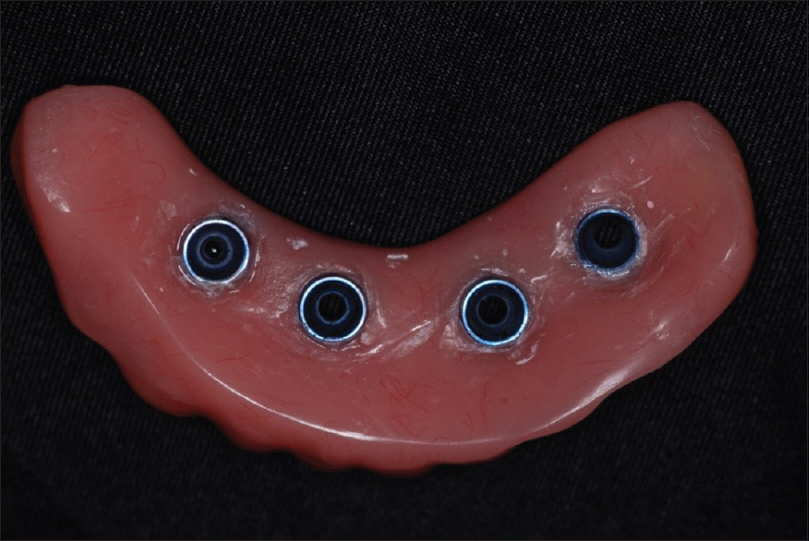 |
Figure 2: Previous mandibular implant-supported complete denture. Observe the gingival over-extension of the flange, which makes the cleaning difficult |
The case was resolved by replacement of that prosthesis by a new mandibular screw-retained implant-supported complete denture, applying the neutral zone technique to establish a more natural positioning of mandibular teeth. The maxillary conventional complete denture was not replaced once it was suitable in terms of esthetic and functional parameters. It was taken an impression of the maxillary complete denture to obtain the maxillary cast that was mounted in a semi adjustable articulator, transferred by face-bow. Open tray impression technique was used to transfer the positions of the mandibular implants, and the impression was poured with type IV dental stone.
A neutral zone record base was made in acrylic resin, and modeling plastic impression compound (Kerr Corp) was softened in a 65°C water bath and attached to the base. The record base was reheated, and seated at the patient’s mouth, and the patient was asked to perform actions of smiling, pursing the lips, sucking, and tongue movements to register a position where buccolingual forces are neutralized.[18]
The maxillary removable complete denture was seated at mouth, and the occlusal excess of compound in the neutral zone record base was selectively cut until reach a proper vertical dimension of occlusion [Figure 3]. The mandible was guided carefully into centric relation and an interocclusal record was made with condensation silicone [Figure 4]. After silicone polymerization, the record base was removed from the mouth, and the mandibular cast was mounted in the semi adjustable articulator.
A comparison between the previous prosthesis with the neutral zone record shows a major invasion of the neutral zone. The [Figure 5] shows the neutral zone base record placed on mandibular definitive cast and the previous implant-supported mandibular complete denture. It can be observed that artificial teeth in the previous implant-supported complete exceeded buccally the neutral zone.
 |
Figure 5: (a) The neutral zone base record placed on mandibular definitive cast; (b) Buccal extension of the previous implant-supported mandibular complete denture exceeding the neutral zone limits |
It was made a lingual and a labial index with condensation silicone over the neutral zone record to guide the teeth mounting on the mandibular definitive cast, limited to the neutral zone. The modeling plastic impression compound was removed from the record base and the index was replaced to establish the space of the neutral zone [Figure 6]. Metal bar fabrication and the teeth arrangement were made respecting the index limits. Waxed trial denture was checked intraorally with regard to occlusal vertical dimension, centric relation, esthetics, and phonetics. The denture was invested, processed, finished and polished using conventional methods. Intraoral views of the new mandibular implant-supported complete denture are shown in [Figure 7]. At 7-day follow-up visit,the clinical inspection revealed no lesions, and the patient reported that he was satisfied with the new prosthesis without any discomfort and phonetic problems [Figure 8].
 |
Figure 6: Lingual and a labial index with condensation silicone delimiting the neutral zone |
 |
Figure 7: Intraoral aspects of the maxillary complete denture and of the new mandibular implant-supported complete denture |
| Discussion |
Developed in 1933,[4] the neutral zone concept is known by different terminologies, including dead zone,[4] stable zone,[7] zone of minimal conflict,[19] zone of least interference,[20] zone of equilibrium,[21] biometric denture space,[22] denture space,[23],[24] and potential denture space.[25] In 1976, the term “neutral zone” was introduced by Beresin and Schiesser,[1] which is the most widely used. The neutral zone term is present in the glossary of prosthodontics terms,[26] defined as “the potential space between the lips and the cheeks on one side and the tongue on the other; that area or position where the forces between the tongue and cheeks or lips are equal”.
In edentulous patients, structures that support lips and cheeks tend to collapse into the oral cavity [10] while tongue has no tendency to atrophy, becoming stronger and hypertrophic, according to the number of teeth missing and presence or absence of dentures.[27] Thus, the natural tooth space is altered [5] when teeth are lost, being defined as denture space.[17] In other words, the neutral zone can be modified along the life, depending of the level of oral cavity collapse. Usually, removable complete dentures are constructed by the conventional technique,[12] which achieves good results. However, neutral zone technique may be helpful in some specific edentulous situations, where the harmony between denture and its surrounding is necessary to provide stability, retention and comfort,[9] such as in severe ridge resorption,[16],[28] severe neurological disorders,[15] Parkinson’s disease,[29] patients undergone to mandibular surgical reconstruction,[13] or partial glossectomy.[14] Some studies showed greater comfort and improved speech clarity,[5] as well as better patient acceptance [12] achieved with neutral zone technique compared with conventional technique to make a complete denture.
In implant-supported prostheses, lack of retention and stability are not a concern, but the respect to with neutral zone limits is important to allow free movement of muscles such as orbicularis oris, buccinators, and tongue which are rhythmically active during chewing and swallowing.[7],[17] If the lower anterior teeth are positioned too far labially, the contraction of the lip will displace the denture posteriorly.[9] In fixed prosthesis, the dislocating will not occur, but it may cause discomfort, oral injuries, tongue and cheek undesirable bites, and limitation of muscle movements, which can affect phonetics.
In this case report, the previous mandibular screw-retained implant-supported complete denture was made in Angle Class I to compensate the accentuated retrognathism. However, the buccal limits of the mandibular incisors exceeded the limit of buccal sulcus, generating discomfort, oral lesions, and phonetic problems. The invasion of neutral zone generates a conflict with the dynamics of the masticatory muscles leading to the denture fail.[11]
| Conclusions |
Although the neutral zone is not a new technique, its use to implant therapy is not well known and disseminated. Thus, it should be indicated also for implant-supported complete denture treatments because it provides a reliable functional pattern for the artificial teeth positioning, leading to a comfort, and better oral functions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References |
| 1. |
Beresin VE, Schiesser FJ. The neutral zone in complete dentures. J Prosthet Dent 1976;36:356-67.
 |
| 2. |
Beresin VE, Schiesser FJ, editors. Neutral Zone in Complete and Partial Dentures. 2nd ed. St. Louis: Mosby; 1979. p. 15, 73-108, 158-83.
|
| 3. |
Fish EW. An analysis of the stabilizing factors in full denture construction. Br Dent J 1931;52:559-70.
|
| 4. |
Fish EW. Using the muscles to stabilize the full lower denture. J Am Dent Assoc 1933;20:2163-9.
|
| 5. |
Fahmy FM, Kharat DU. A study of the importance of the neutral zone in complete dentures. J Prosthet Dent 1990;64:459-62.
|
| 6. |
Khamis M, Razek A, Abdalla F. Two-dimensional study of the neutral zone at different occlusal vertical heights. J Prosthet Dent 1981;46:484-9.
|
| 7. |
Brill N, Tryde G, Cantor R. The dynamic nature of the lower denture space. J Prosthet Dent 1965;15:401-18.
|
| 8. |
Schiesser FJ. The neutral zone and polished surfaces in complete dentures. J Prosthet Dent 1964;14:854-65.
|
| 9. |
Gahan MJ, Walmsley AD. The neutral zone impression revisited. Br Dent J 2005;198:269-72.
|
| 10. |
Porwal A, Sasaki K. Current status of the neutral zone: A literature review. J Prosthet Dent 2013;109:129-34.
|
| 11. |
Russell AF. The reciprocal lower complete denture. J Prosthet Dent 1959;9:180-90.
|
| 12. |
Barrenäs L, Odman P. Myodynamic and conventional construction of complete dentures: A comparative study of comfort and function. J Oral Rehabil 1989;16:457-65.
|
| 13. |
Kokubo Y, Fukushima S, Sato J, Seto K. Arrangement of artificial teeth in the neutral zone after surgical reconstruction of the mandible: A clinical report. J Prosthet Dent 2002;88:125-7.
|
| 14. |
Ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutral zone approach for denture fabrication for a partial glossectomy patient: A clinical report. J Prosthet Dent 2000;84:390-3.
|
| 15. |
Karkazis HC. Prosthodontic management of a patient with neurological disorders after resection of an acoustic neurinoma: A clinical report. J Prosthet Dent 2002;87:419-22.
|
| 16. |
Wee AG, Cwynar RB, Cheng AC. Utilization of the neutral zone technique for a maxillofacial patient. J Prosthodont 2000;9:2-7.
|
| 17. |
Cagna DR, Massad JJ, Schiesser FJ. The neutral zone revisited: From historical concepts to modern application. J Prosthet Dent 2009;101:405-12.
|
| 18. |
Makzoumé JE. Morphologic comparison of two neutral zone impression techniques: A pilot study. J Prosthet Dent 2004;92:563-8.
|
| 19. |
Matthews E. The polished surfaces. Br Dent J 1961;111:407-11.
|
| 20. |
Wright SM. The polished surface contour: A new approach. Int J Prosthodont 1991;4:159-63.
|
| 21. |
Grant AA, Johnson W. An introduction to removable denture prosthetics. Edinburgh: Churchill Livingstone; 1983. p. 24-8.
|
| 22. |
Watt DM, MacGregor AR. Designing Complete Dentures. 2nd ed: Oxford: Butterworth-Heinemann; 1986. p. 54-69.
|
| 23. |
Heath R. A study of the morphology of the denture space. Dent Pract Dent Rec 1970;21:109-17.
|
| 24. |
Schlosser RO. Complete denture prosthesis. Philadelphia: WB Saunders; 1939. p. 183-90.
|
| 25. |
Roberts AL. The effects of outline and form upon denture stability and retention. Dent Clin North Am 1960;4:293-303.
|
| 26. |
The glossary of prosthodontic terms. J Prosthet Dent 2005;94:10-92.
|
| 27. |
Rinald P, Sharry J. Tongue force and fatigue in adults. J Prosthet Dent 1963;13:857-65.
|
| 28. |
Yeh YL, Pan YH, Chen YY. Neutral zone approach to denture fabrication for severe mandibular ridge resorption patient: Systematic review and modern technique. J Dent Sci 2013;8:432-8.
|
| 29. |
Makzoume JE. Complete denture prosthodontics for a patient with Parkinson’s disease using the neutral zone concept: A clinical report. Gen Dent 2008;56:12-6.
|
| Figures |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8]
|